NEXIUM MUPS Tablet
ក្រុមហ៊ុនផលិតឱសថ:
Astra Zeneca AB, Sweden
ក្រុមហ៊ុនចែកចាយឱសថនៅប្រទេសកម្ពុជា:
DKSH


- សារធាតុសកម្ម
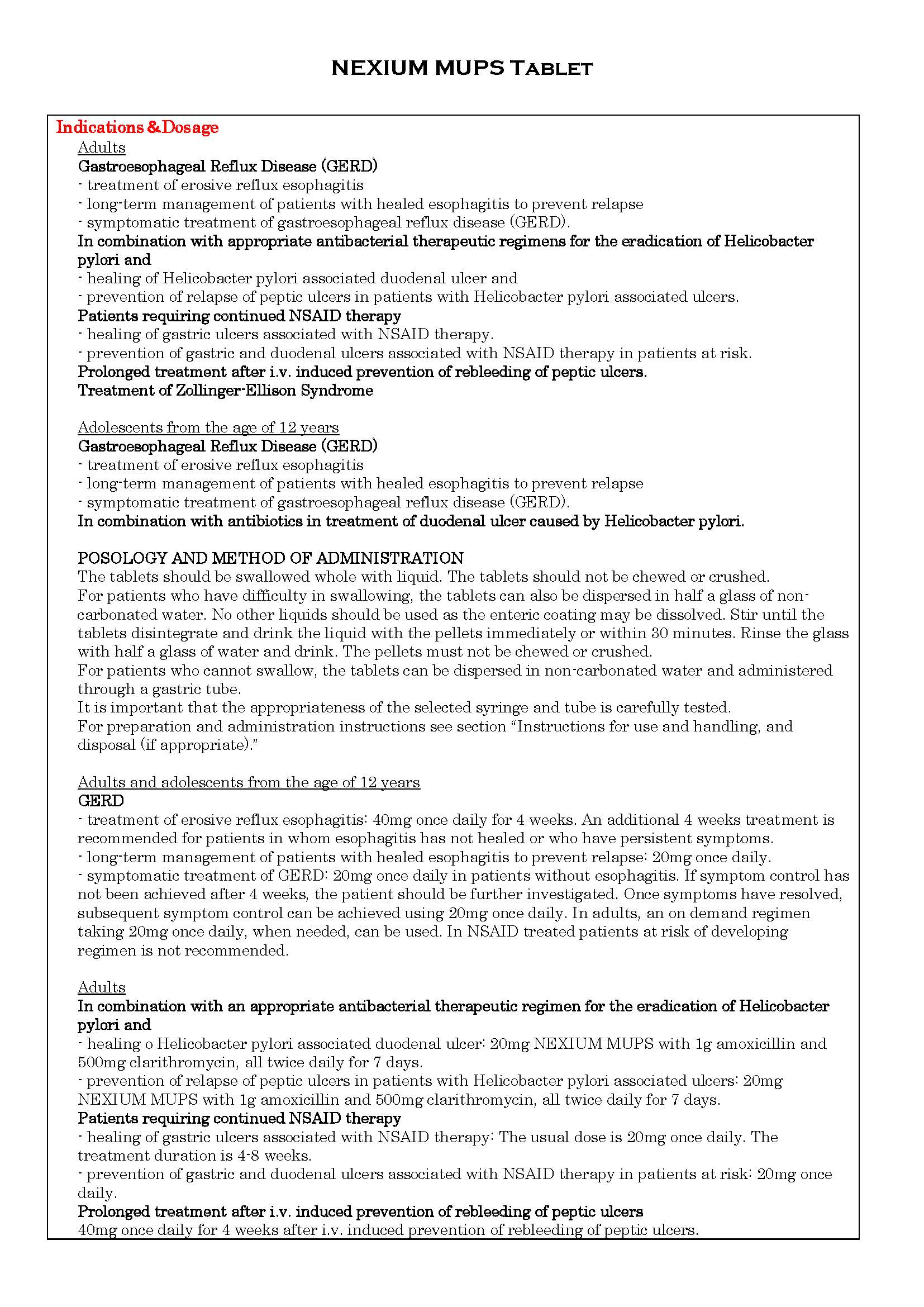
- ប្រសិទ្ធិភាពព្យាបាល និង កម្រិតប្រើប្រាស់
- ហាមប្រើ
- ផលរំខាន
- អន្តរប្រតិកម្ម
- ស្ត្រីមានផ្ទៃពោះ និង ស្ត្រីបំបៅដោះកូន
- ការប្រុងប្រយ័ត្នជាពិសេស
- សកម្មភាពឱសថ បរិយាយប័ណ្ណឱសថ
-
សារធាតុសកម្ម
-
ប្រសិទ្ធិភាពព្យាបាល និង កម្រិតប្រើប្រាស់

-
ហាមប្រើ
ហាមប្រើ៖
- អ្នកជំងឺងាយមានប្រតិកម្មជាមួយឱសថនេះ និងសារធាតុផ្សំណាមួយ រួមទាំង ឱសថ Benzimidazole។
- ហាមប្រើប្រាស់ព្រមគ្នាជាមួយឱសថ Nelfinavir។Known hypersensitivity to esomeprazole, substituted benzimidazoles or any other constituents of the formulation. Esomeprazole should not be used concomitantly with nelfinavir, atazanavir.
-
ផលរំខាន
ផលរំខានរួមមាន៖
- វិបត្តិឈាម និងប្រព័ន្ធទឹករងៃ: គ្រាប់ឈាមសតិចជាងធម្មតា ប្លាកែតថយចុះ ការថយចុះកោសិកាគ្រប់មុខក្នុងឈាម (កម្រណាស់)
- វិបត្តិប្រព័ន្ធភាពស៊ាំ : គ្រុនក្ដៅ ហើមសរសៃឈាម ប្រតិកម្មស្ហុកanaphylatic (កម្រណាស់)
- វិបត្តិការបំលែងចំណីអាហារ : (ហើមជាលិកា ពិសេសហើមចុងដៃ ចុងជើង) កង្វះជាតិសូដ្យូមក្នុងឈាម (កម្រណាស់)
- វិបត្តិផ្លូវចិត្ត: ដេកមិនលក់ ញ័រខ្លួន ភ័ន្តភាំងស្មារតី គឃ្លើន រវើរវាយ (កម្រ)
- វិបត្តិសរសៃប្រសាទ: ឈឺក្បាល វិលមុខ ស្ពឹក ដេកមិនលក់ វិបត្តិរសជាតិ (កម្រ)
- វិបត្តិគំហើញ: ស្រវាំងភ្នែក (កម្រ)
- វិបត្តិត្រចៀក និងផ្នែកក្នុង: ធីងធោង (កម្រ)
- វិបត្តិផ្លូវដង្ហើម: ទងសួតរួមតូច (កម្រ)
- វិបត្តិក្រពះ-ពោះវៀន : ឈឺពោះ ទល់លាមក រាក ភើ ចង្អោរ ក្អួត ស្ងួតមាត់ រលាកមាត់ ដុះមេរោគផ្សិតក្នុងក្រពះ-ពោះវៀន(កម្រ)
- វិបត្តិថ្លើម-ទឹកប្រមាត់: អង់ស៊ីមថ្លើមកើន រលាកថ្លើម ឬ រលាកថ្លើមជាមួយការកើតជំងឺខាន់លឿង ខ្សោយមុខងារថ្លើម ជម្ងឺរលាកខួរក្បាល (កម្រ)
- វិបត្តិស្បែកនិងជាលិកាក្រោមស្បែក : រលាកស្បែកដោយរមាស់ រមាស់កន្ទួលលើស្បែក កន្ទាលត្រអាក ជ្រុះសក់ ប្រតិកម្មដោយពន្លឺ ពងទឹកលើស្បែក ប្រតិកម្មអាលែកហ្ស៊ីធ្ងន់ធ្ងរដោយមានកន្ទួលលើស្បែក និងជាលិកាទន់(Steven Johnson) រលួយស្បែកដោយជាតិពុល (កម្រណាស់)
- វិបត្តិសាច់ដុំនិងឆ្អឹង: ឈឺសន្លាក់ដៃជើង ឈឺចាប់សាច់ដុំ ខ្សោយសាច់ដុំ (កម្រណាស់)
- វិបត្តិតម្រងនោម និងផ្លូវនោម: រលាកតម្រងនោម ចន្លោះកោសិកាណេហ្វ្រុង (កម្រ)
- វិបត្តិប្រព័ន្ធបន្តពូជ និងដោះ : ដោះរីកធំមិនធម្មតា (កម្រណាស់)
- វិបត្តិទូទៅ : រសេះរសោះ បែកញើស (កម្រ) និង ធ្វើអោយមានការថយចុះកំរិតម៉ាញ៉េស្យូមក្នុងឈាម។Headache, abdominal pain, diarrhoea and nausea are among those adverse reactions that have been most commonly reported in clinical trials (and also from post-marketing use). In addition, the safety profile is similar for different formulations, treatment indications, age groups and patient populations.
The following adverse drug reactions have been identified or suspected in the clinical trials programme for esomeprazole and post-marketing. None was found to be dose-related.
Blood and lymphatic system disorders
Rare: Leukopenia, thrombocytopenia
Very rare: Agranulocytosis, pancytopenia
Immune system disorders
Rare: Hypersensitivity reactions e.g. fever, angioedema and anaphylactic reaction/shock
Metabolism and nutrition disorders
Uncommon: peripheral oedema
Rare: Hyponatraemia
Not known: Hypomagnesaemia; severe hypomagnesaemia can correlate with hypocalcaemia. Hypomagnesaemia may also result in hypokalaemia.
Psychiatric disorders
Uncommon: Insomnia
Rare: Agitation, confusion, depression
Very rare: Aggression, hallucinations
Nervous system disorders
Common: Headache
Uncommon: Dizziness, paraesthesia, somnolence
Rare: Taste disturbance
Eye disorders
Rare: Blurred vision
Ear and labyrinth disorders
Uncommon: Vertigo
Respiratory, thoracic and mediastinal disorders
Rare: Bronchospasm
Gastrointestinal disorders
Common: Abdominal pain, constipation, diarrhoea, flatulence, nausea/vomiting
Uncommon: Dry mouth
Rare: Stomatitis, gastrointestinal candidiasis
Not known: Microscopic colitis
Hepatobiliary disorders
Uncommon: Increased liver enzymes
Rare: Hepatitis with or without jaundice
Very rare: Hepatic failure, encephalopathy in patients with pre-existing liver disease
Skin and subcutaneous tissue disorders
Uncommon: Dermatitis, pruritus, rash, urticaria
Rare: Alopecia, photosensitivity
Very rare: Erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis (TEN)
Musculoskeletal and connective tissue disorders
Uncommon: Fracture of the hip, wrist or spine
Rare: Arthralgia, myalgia
Very rare: Muscular weakness
Renal and urinary disorders
Very rare: Interstitial nephritis; in some patients renal failure has been reported concomitantly.
Reproductive system and breast disorders
Very rare: Gynaecomastia
General disorders and administration site conditions
Rare: Malaise, increased sweating
-
អន្តរប្រតិកម្ម
អន្តរកម្មឱសថ
- ក្នុងករណីប្រើឱសថនេះរួមជាមួយឱសថផ្សេងទៀតដូចជាឱសថ Clarithromycin និង Cisapride ដើម្បីការព្យាបាលជំងឺដំបៅចុងក្រពះ និងគល់ពោះវៀនតូច (Helicobacter Pylori) ត្រូវគិតគូរដល់ការហាមប្រើ និងអន្តរកម្មរបស់ឱសថដែលត្រូវប្រើរួមគ្នាទាំងនេះ។
- ការប្រើឱសថនេះរួមជាមួយឱសថ Ketoconazole និង ឱសថ Itraconazole បន្ថយការជ្រាបចូលទៅក្នុងសរសៃឈាមពីពោះវៀនតូចនៃឱសថដែលត្រូវរួមគ្នាទាំងនេះ។
- ការប្រើឱសថនេះរួមជាមួយឱសថ Diazepam ឱសថPhenytoin និង ឱសថWarfarin ពន្យារការបញ្ចេញចោលនៃកំហាប់ ឱសថដែលត្រូវប្រើរួមគ្នាទាំងនេះ។
- ឱសថនេះមានប្រតិកម្មជាមួយពួក Digoxin, protease inhibitors, atazanavir, clopidogrel និងឱសថដែលមានឥទ្ធិពលចំពោះ CYP2C19 ឬ CYP3A4។Interaction studies have only been performed in adults.
(See the package insert about the details.)
Medicinal products with pH dependent absorption (ketoconazole, itraconazole, erlotinib)(digoxin).
Some protease inhibitors
Atazanavir 300mg/Ritonavir 100mg
Drugs metabolised by CYP2C19 (diazepam, citalopram, imipramine, clomipramine, phenytoin)
Warfarin-treated patients
Cisapride
Esomeprazole has been shown to have no clinically relevant effects on the pharmacokinetics of amoxicillin or quinidine.
Studies evaluating concomitant administration of esomeprazole and either naproxen or rofecoxib did not identify any clinically relevant pharmacokinetic interactions during short-term studies.
Clopidogrel
Unknown mechanism
Tacrolimus
Methotrexate
Effects of other drugs on the pharmacokinetics of esomeprazole
CYP3A4 inhibitor (clarithromycin)(voriconazole)
Drugs known to induce CYP2C19 or CYP3A4 or both (such as rifampicin, St. John’s wort)
-
ស្ត្រីមានផ្ទៃពោះ និង ស្ត្រីបំបៅដោះកូន
ស្ត្រីបំបៅកូន: គួរជៀសវាងប្រើឱសថនេះ។
Clinical data on exposed pregnancies are insufficient. With the racemic mixture omeprazole, data on a larger number of exposed pregnancies from epidemiological studies indicate no malformative nor fetotoxic effect. Animal studies with esomeprazole do not indicate direct or indirect harmful effects with respect to embryonal/fetal development. Animal studies with the racemic mixture do not indicate direct or indirect harmful effects with respect to pregnancy, parturition or postnatal development. Caution should be exercised when prescribing to pregnant women.
It is not known whether esomeprazole is excreted in human breast milk. No studies in lactating women have been performed. Therefore NEXIUM MUPS should not be used during breast-feeding.
-
ការប្រុងប្រយ័ត្នជាពិសេស
ការប្រុងប្រយ័ត្ន៖
- ក្នុងករណីកើតមាន៖ ការស្រកទម្ងន់ ការក្អួត ពិបាកលេបអាហារ ក្អួតធ្លាក់ឈាម ឬលាមកពណ៌ខ្មៅ ដំបៅក្រពះ ឬ មហារីកក្រពះ មិនគួរប្រើឱសថនេះទេ។
- ការប្រើឱសថនេះរយៈពេលលើសពី1ឆ្នាំ គួរតាមដានរោគសញ្ញាប្រសិនបើមានអាការៈប្លែកត្រូវពិគ្រោះជាមួយគ្រូពេទ្យ។
- គួរជៀសវាងប្រើឱសថនេះ ចំពោះអ្នកជំងឺដេលសរីរាង្គមិនទទួលជាតិស្ករ Fructose មិនជ្រាបជាតិស្ករ Glucose-gelactose ឬ ខ្វះអង់ស៊ីម Sucrase-isomaltase។
- គួរជៀសវាងប្រើឱសថនេះ ពេលព្រមគ្នាជាមួយក្រុមឱសថ Atazanavir, CYP2C19 ដែលជាអ្នករារាំងនិងបង្អាក់ជាមួយ Laboratory tests។In the presence of any alarm symptom (e.g. significant unintentional weight loss, recurrent vomiting, dysphagia, haematemesis or melaena) and when gastric ulcer is suspected or present, malignancy should be excluded, as treatment with NEXIUM MUPS may alleviate symptoms and delay diagnosis.
Patients on long-term treatment (particularly those treated for more than a year) should be kept under regular surveillance.
Patients on on-demand treatment should be instructed to contact their physician if their symptoms change in character. When prescribing esomeprazole for on demand therapy, the implications for interactions with other pharmaceuticals, due to fluctuating plasma concentrations of esomeprazole should be considered.
When prescribing esomeprazole for eradication of Helicobacter pylori possible drug interactions for all components in the triple therapy should be considered. Clarithromycin is a potent inhibitor of CYP3A4 and hence contraindications and interactions for clarithromycin should be considered when the triple therapy is used in patients concurrently taking other drugs metabolised via CYP3A4 such as cisapride.
This medicinal product contains sucrose. Patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrose-isomaltase insufficiency should not take this medicine.
Treatment with PPIs may lead to slightly increased risk of gastrointestinal infections such as Salmonella and Campylobacter.
Co-administration of esomeprazole with atazanavir is not recommended. If the combination of atazanavir with a PPI is judged unavoidable, close clinical monitoring is recommended in combination with an increase in the dose of atazanavir to 400mg with 100mg of ritonavir; esomeprazole 20mg should not be exceeded.
Esomeprazole, as all acid-blocking medicines, may reduce the absorption of vitamin B12 (cyanocobalamin) due to hypo- or achlorhydria. This should be considered in patients with reduced body stores or risk factors for reduced vitamin B12 absorption on long-term therapy.
Esomeprazole is a CYP2C19 inhibitor. When starting or ending treatment with esomeprazole, the potential for interactions with drugs metabolised through CYP2C19 should be considered. An interaction is observed between clopidogrel and esomeprazole. The clinical relevance of this interaction is uncertain. As a precaution, concomitant use of esomeprazole and clopidogrel should be discouraged.
Severe hypomagnesaemia has been reported in patients treated with PPIs for at least 3 months, and in most cases for a year. Serious manifestations of hypomagnesaemia such as fatigue, tetany, delirium, convulsions, dizziness and ventricular arrhythmia can occur but they may begin insidiously and be overlooked. In most affected patients, hypomagnesaemia improved after magnesium replacement and discontinuation of the PPI.
For patients expected to be on prolonged treatment or who take PPIs with digoxin or drugs that may cause hypomagnesaemia (e.g. diuretics), healthcare professionals should consider measuring magnesium levels before starting PPI treatment and periodically during treatment.
PPIs, especially if used in high doses and over long durations (>1 year), may modestly increase the risk of hip, wrist and spine fracture, predominantly in the elderly or in presence of other recognised risk factors. Observational studies suggest that PPIs may increase the overall risk of fracture by 10-40%. Some of this increase may be due to other risk factors. Patients at risk of osteoporosis should receive care according to current clinical guidelines and they should have an adequate intake of vitamin and calcium.
Interfere with laboratory tests
Increased Chromogranin A (CgA) level may interfere with investigations for neuroendocrine tumors. To avoid this interference, esomeprazole treatment should be stopped for at least 5 days before CgA measurements.
-
សកម្មភាពឱសថ
Esomeprazole is the S-isomer of omeprazole and reduces gastric acid secretion through a specific targeted mechanism of action. It is a specific inhibitor of the acid pump in the parietal cell. Both the R- and S-isomer of omeprazole have similar pharmacodynamic activity.
Site and mechanism of action
Esomeprazole is a weak base and is concentrated and converted to the active form in the highly acidic environment of the secretory canaliculi of the parietal cell, where it inhibits the enzyme H+K+-ATPase - the acid pump and inhibits both basal and stimulated acid secretion.
*ព័ត៌មានឱសថត្រូវបានរៀបរៀងដោយ អ៊ីម៉ាតុគឹ មេឌីក (ខេមបូឌា) ដោយផ្អែកលើប្រភពព័ត៌មានខាងក្រោម។ សម្រាប់ព័ត៌មានលម្អិត សូមស្វែងរកនៅក្នុងក្រដាសព័ត៌មាននៃឱសថនីមួយៗ ឬ សាកសួរទៅកាន់ក្រុមហ៊ុនឱសថឬតំណាងចែកចាយនៃឱសថនីមួយៗ។
ប្រភពព័ត៌មាន៖
- ក្រដាសព័ត៌មាននៃឱសថសម្រាប់អ្នកជំនាញវេជ្ជសាស្ត្រដែលប្រើប្រាស់នៅប្រទេសជប៉ុន (Pharmaceutical and Medical Devices Agency, Pmda): https://www.pmda.go.jp
- ព័ត៌មានសង្ខេបនៃឱសថសម្រាប់អ្នកជំងឺដែលប្រើប្រាស់នៅប្រទេសជប៉ុន: http://www.rad-ar.or.jp